

EMT respiratory A&p
ANATOMY
1
For anatomy, you must be able to name, label, pronounce and describe the location and function of the following:
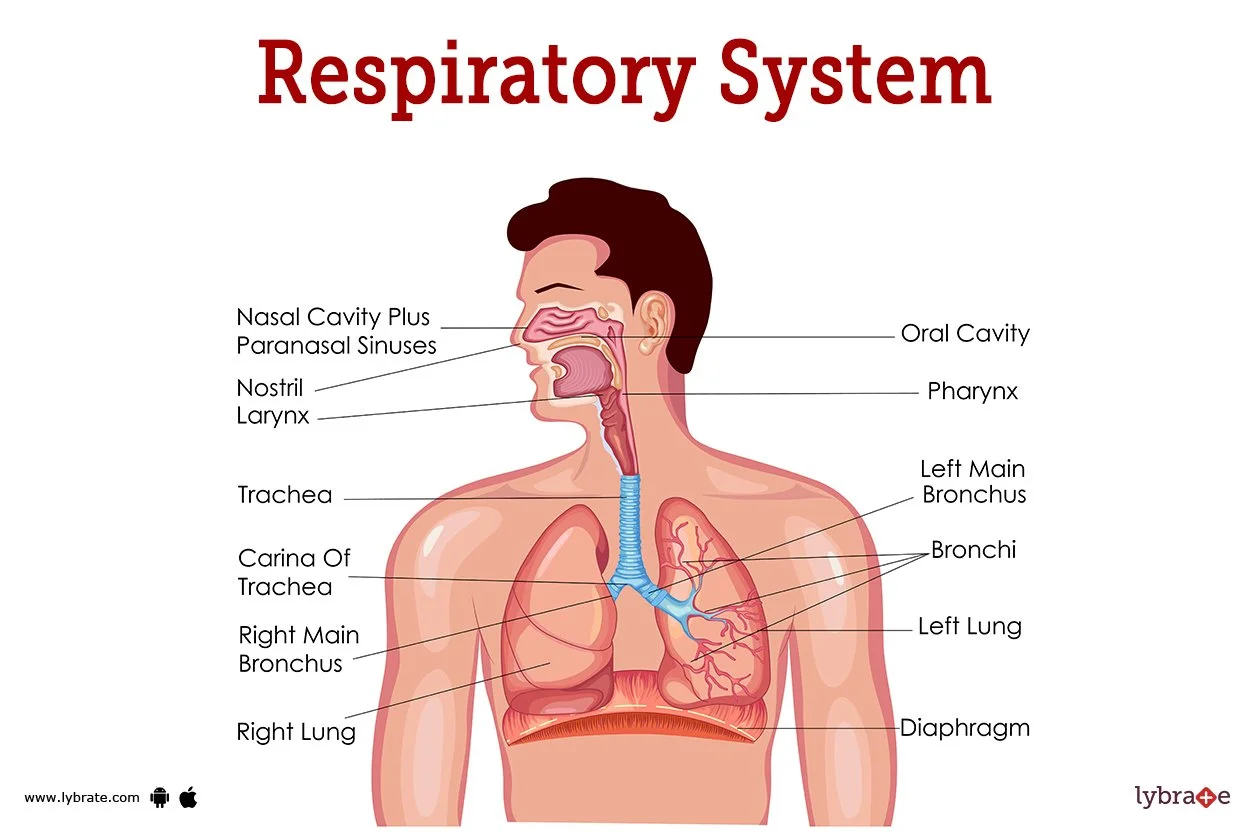
Upper airway structures:
Nasal cavity
Oral cavity
Pharynx (nasopharynx, oropharynx, laryngopharynx)
Larynx
Epiglottis
Lower airway structures:
Trachea
Right and left main bronchi
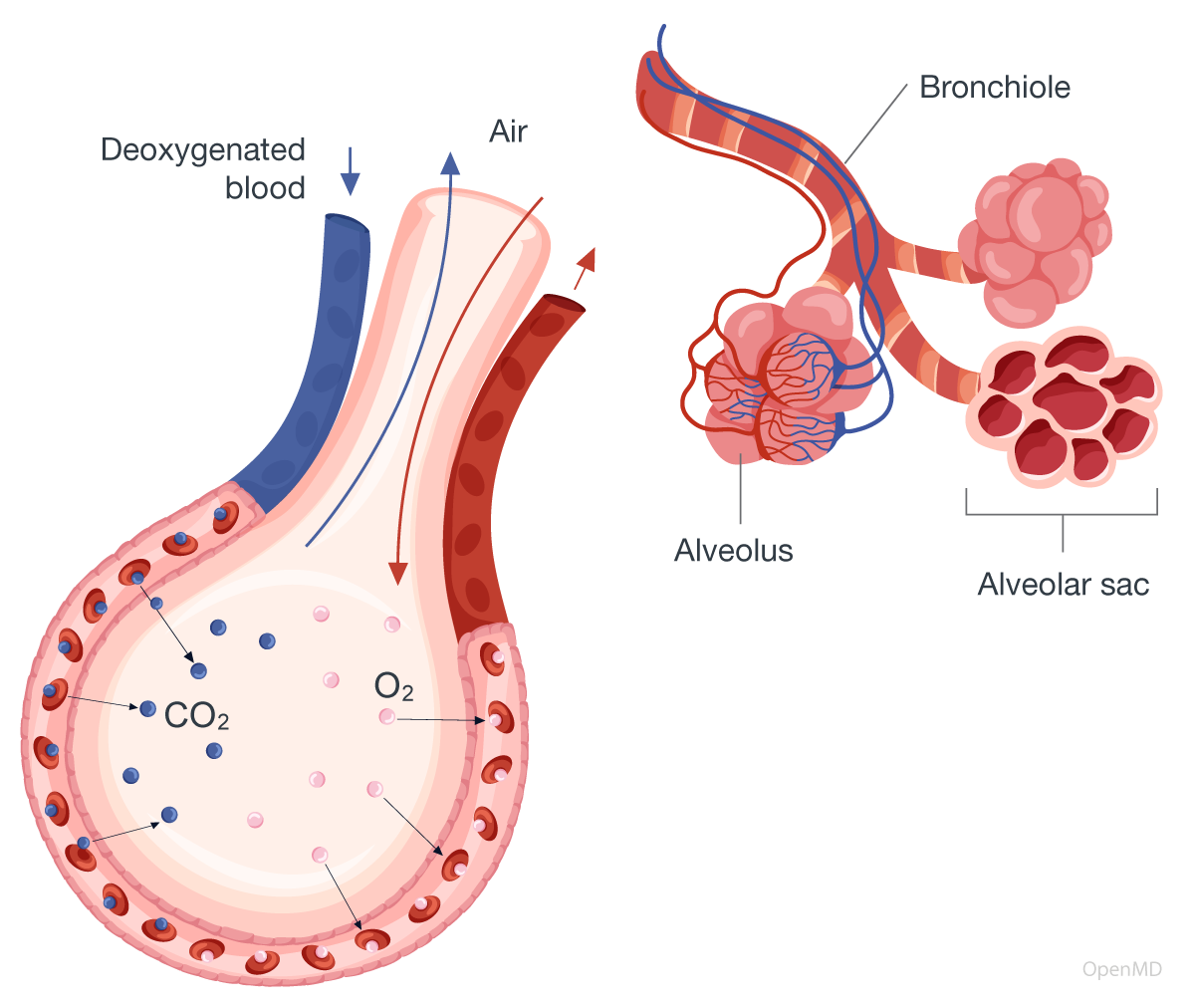
Bronchioles
Alveoli
Lungs:
Right lung (3 lobes)
Left lung (2 lobes)
Hilum
Pleura:
Visceral pleura
Parietal pleura
Pleural space
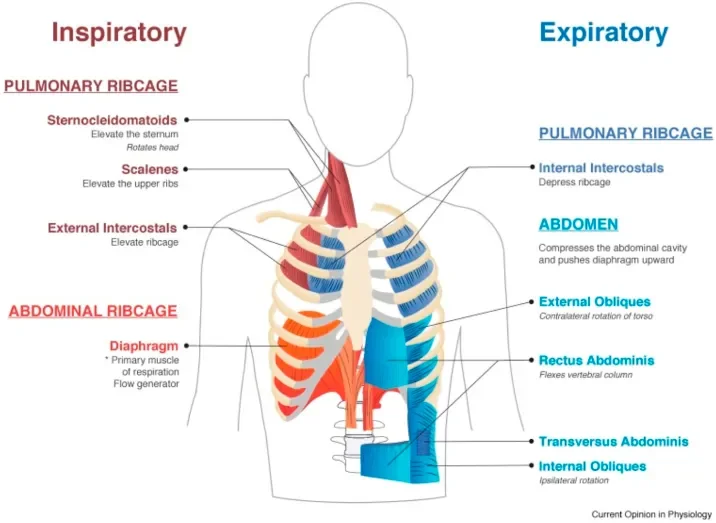
Respiratory muscles:
Diaphragm
Intercostal muscles
Thoracic structures relevant to breathing:
Rib cage
Mediastinum (conceptually)
You must understand the difference between:
Upper vs lower airway
Conducting zone vs gas exchange zone
Ventilation structures vs perfusion structures
For physiology, you should be able to understand the underlying pathophysiology behind:
Ventilation mechanics:
How the human body knows when to breath in health and with COPD (hypercapnia vs hypoxic drive)
Role of diaphragm contraction
Inspiration vs expiration
Accessory muscle use
Gas exchange:
Diffusion at the alveolar-capillary membrane
Oxygen loading and carbon dioxide unloading
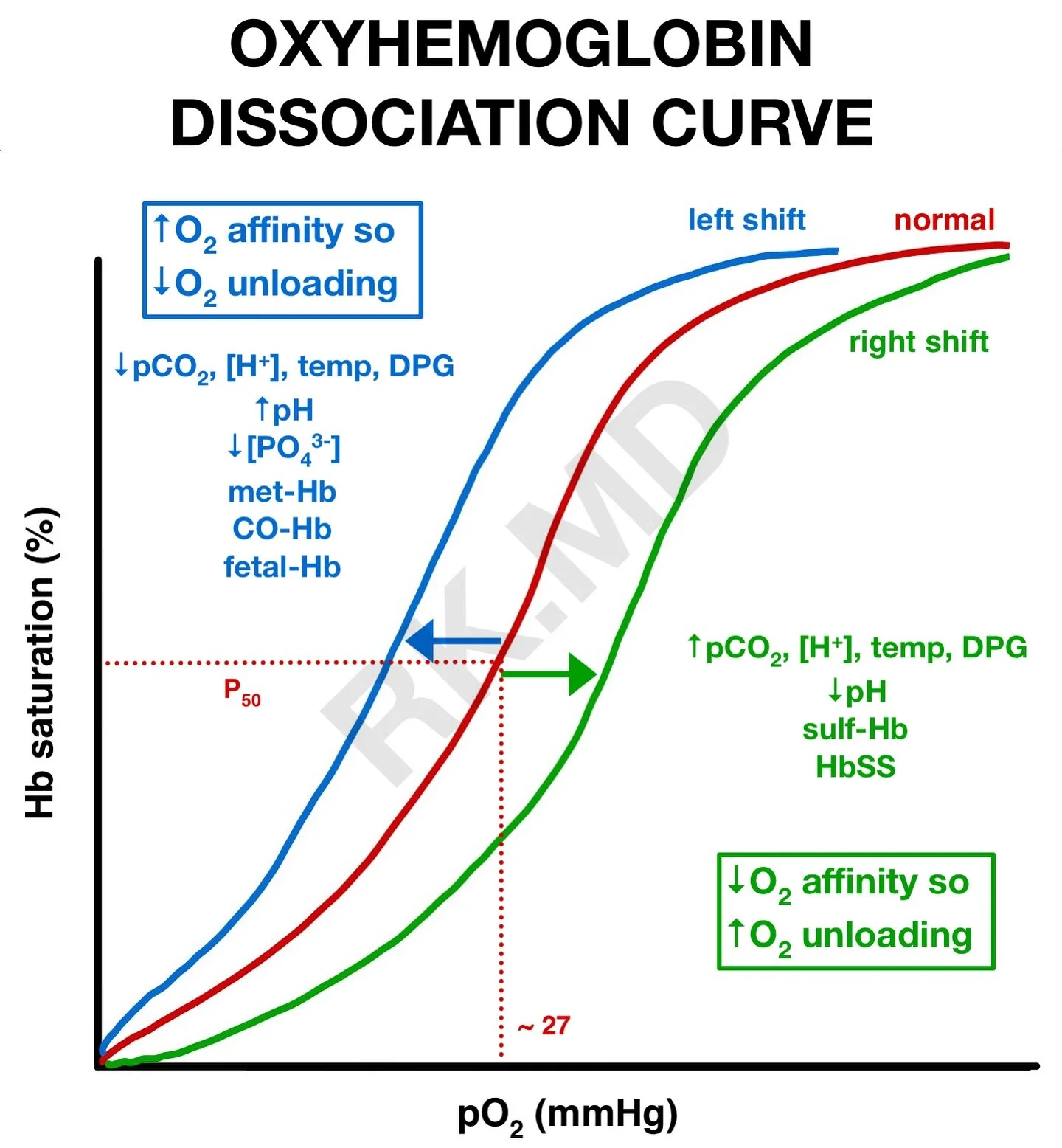
Oxygen transport:
Haemoglobin binding
Oxyhaemoglobin dissociation curve (conceptual only — left/right shift awareness)
Carbon dioxide transport (basic overview):
Dissolved CO₂
Bound to haemoglobin
Ventilation–perfusion (V/Q) matching:
What happens when ventilation fails
What happens when perfusion fails
Why both are required
Hypoxia vs hypoxaemia:
Low tissue oxygen vs low blood oxygen
Hypercapnia and respiratory acidosis (basic mechanism)
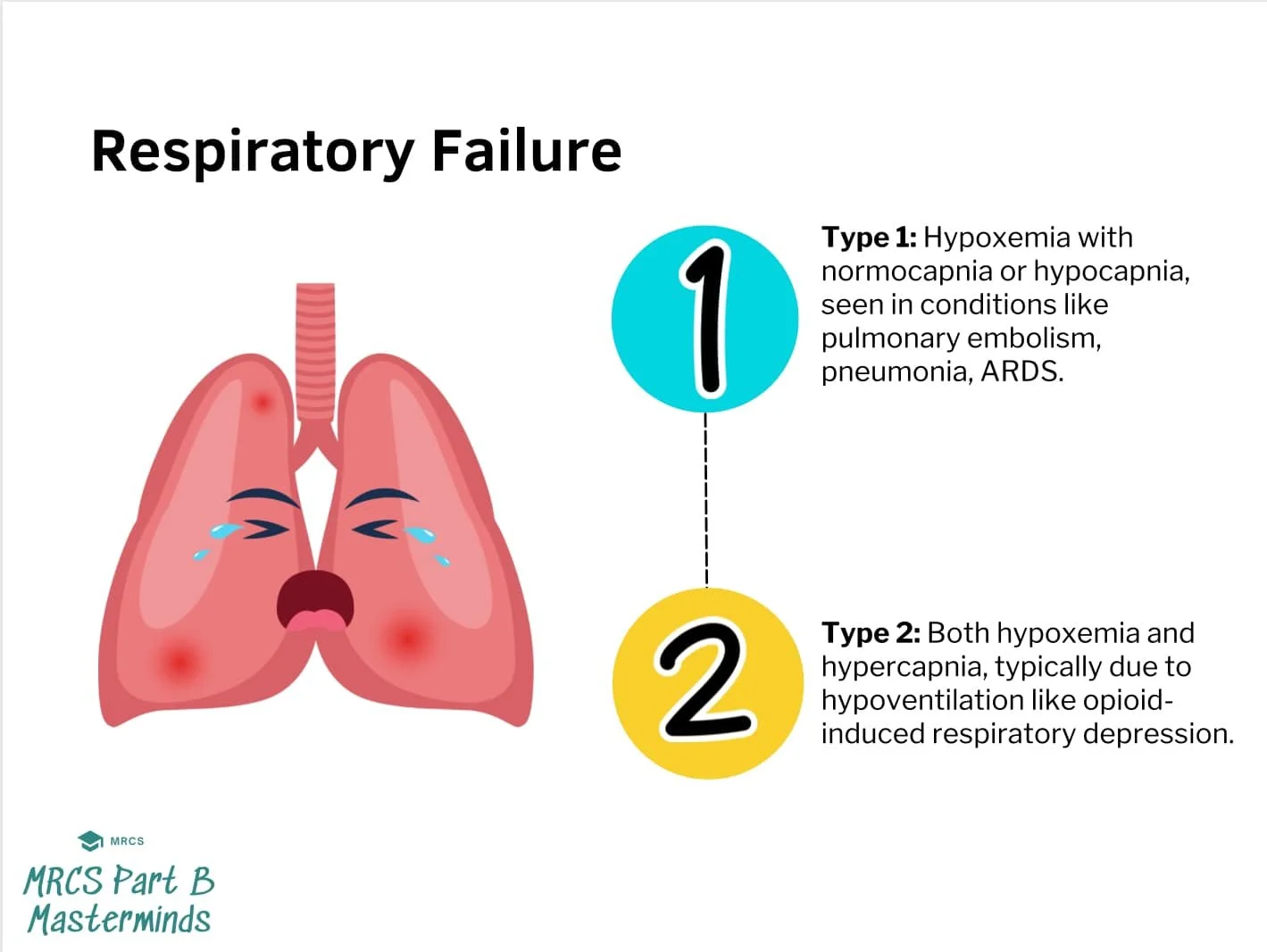
Respiratory failure:
Type 1 respiratory failure (low O₂)
Type 2 respiratory failure (low O₂ + high CO₂)
Obstructive vs restrictive respiratory diseases/injuries:
Asthma
COPD (emphysema and bronchitis in particular)
Anaphylaxis
Foreign body obstruction
Pulmonary oedema
Pneumothorax
Tension pneumothorax
Pulmonary embolism
Pneumonia
You must understand the progression of:
Airway obstruction → hypoxaemia → hypoxia → organ failure → cardiac arrest
Exacerbation of disease → poor ventilation → increased effort of breathing → fatigue → CO₂ retention → decompensation → organ failure → cardiac arrest
Respiratory tract Infection → inflammation → consolidation → impaired gas exchange → respiratory failure → organ failure → cardiac arrest
PHYSIOLOGY
2
Why do emt’s need to know this?
3
Shortness of breath is one of the most common ambulance presentations. Without a strong understanding of respiratory anatomy and physiology, assessment becomes guesswork.
Airway assessment relies on knowing:
Where obstruction can occur
How airway positioning improves patency
When airway adjuncts are appropriate
Breathing assessment depends on understanding:
Why respiratory rate changes
Why accessory muscles matter
Why silent chest in asthma is a red flag
Why unequal chest rise suggests pneumothorax
Oxygen therapy decisions require insight into:
Hypoxia vs hypercapnia
When high-flow oxygen is essential
Why some COPD patients retain CO₂
When ventilatory support is needed rather than just oxygen
Recognising life-threatening patterns such as the following requires understanding what is failing; ventilation, perfusion, or both:
Tension pneumothorax
Severe asthma exhaustion
Anaphylaxis airway compromise
Pulmonary embolism
Remember: symptoms such as agitation, confusion and reduced GCS can all be respiratory in origin. Misinterpreting these as purely neurogenic or cardiogenic for example, can delay life-saving airway management and breathing support.
Differentiating between:
Anxiety hyperventilation
Asthma exacerbation
Acute pulmonary oedema
Sepsis-related tachypnoea
Opioid-induced respiratory depression
…directly affects whether a patient is:
Managed on scene
Given immediate drug therapy
Ventilated
Transported urgently under blue lights
Respiratory compromise deteriorates quickly. EMTs must recognise the early physiological warning signs before cardiac arrest occurs.
Ultimately, respiratory A&P allows you to answer three critical questions on scene:
Is oxygen getting in?
Is oxygen getting into the blood?
Is oxygen getting to the tissues?
If you understand those three steps clearly, your respiratory assessment becomes structured, confident and clinically safe.