

EMT neurology A&p
ANATOMY
1
For anatomy, you must be able to name, label, pronounce and describe the location and function of the following:
Central Nervous System (CNS):
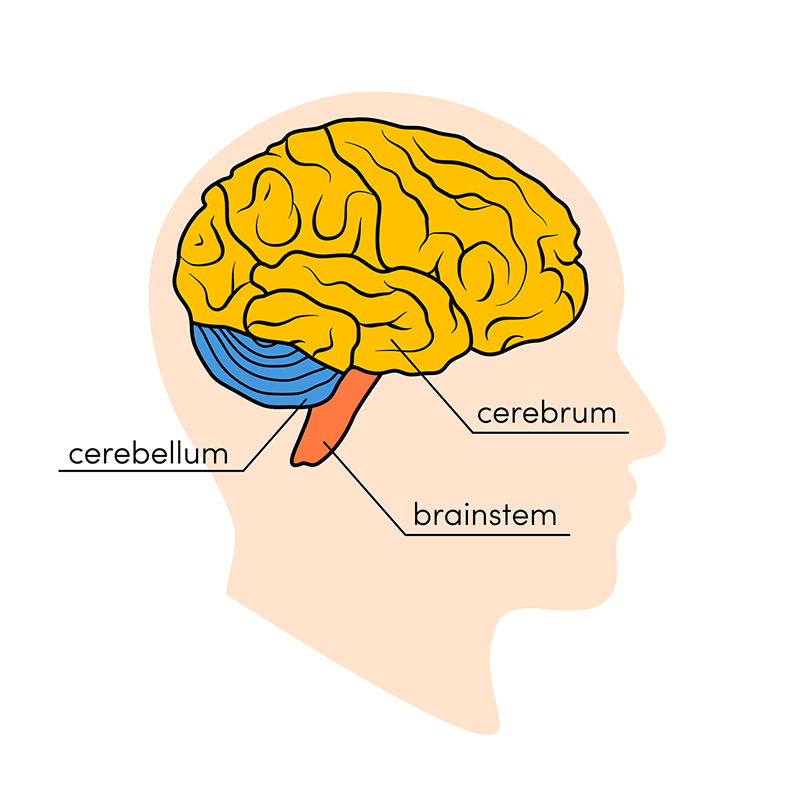
Brain:
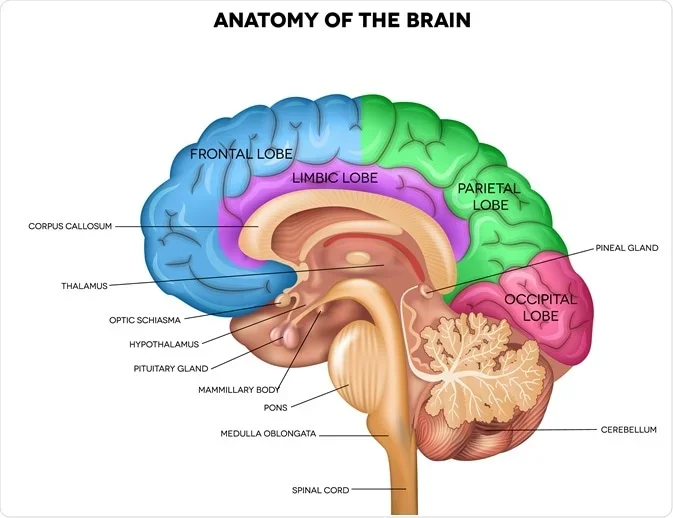
Cerebrum:
Frontal lobe
Parietal lobe
Temporal lobe
Occipital lobe
Cerebral cortex
Central sulcus
Parieto-occipital sulcus
Corpus callosum
Thalamus
Hypothalamus
Pituitary gland
Pineal gland
Optic chiasma
Lateral ventricles
Third ventricle
Choroid plexus
Cerebellum
Brainstem
Midbrain
Pons
Medulla oblongata
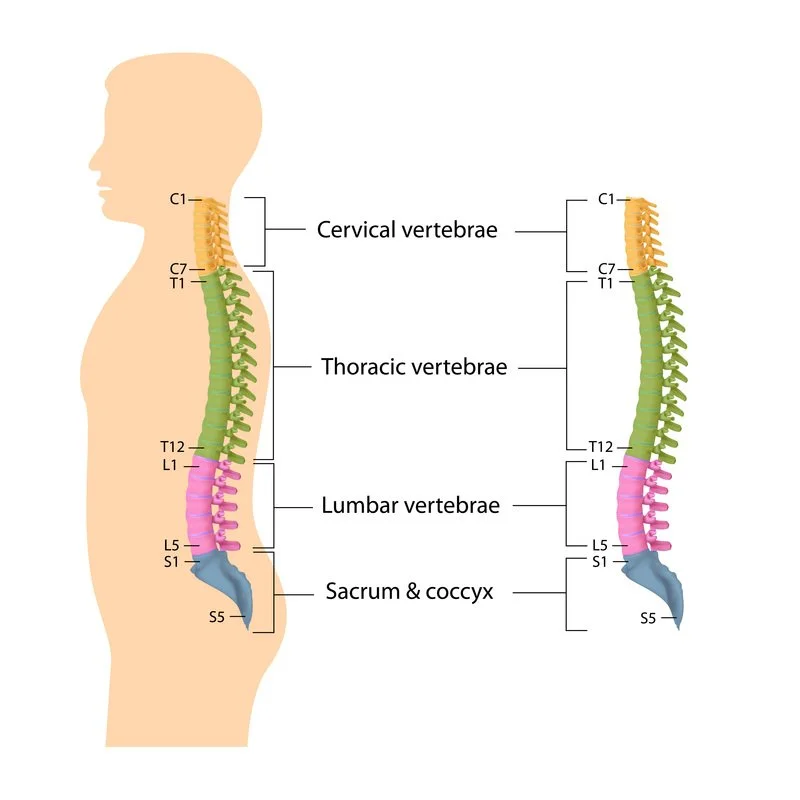
Spinal cord
Cervical region
Thoracic region
Lumbar region
Sacral region
Protective structures:
Skull
Meninges (dura mater, arachnoid mater, pia mater)
Cerebrospinal fluid (CSF)
Peripheral Nervous System (PNS):
Two main subdivisions:
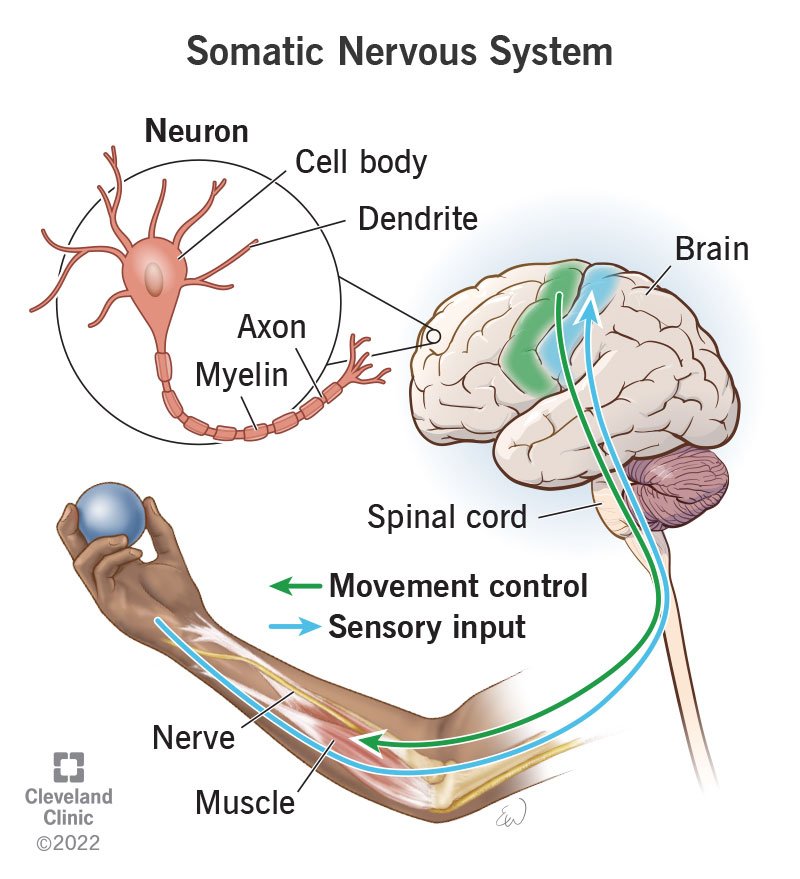
Somatic Nervous System (Voluntary control):
Sensory nerves (afferent)
Association nerves (interneurons)
Motor nerves (efferent)
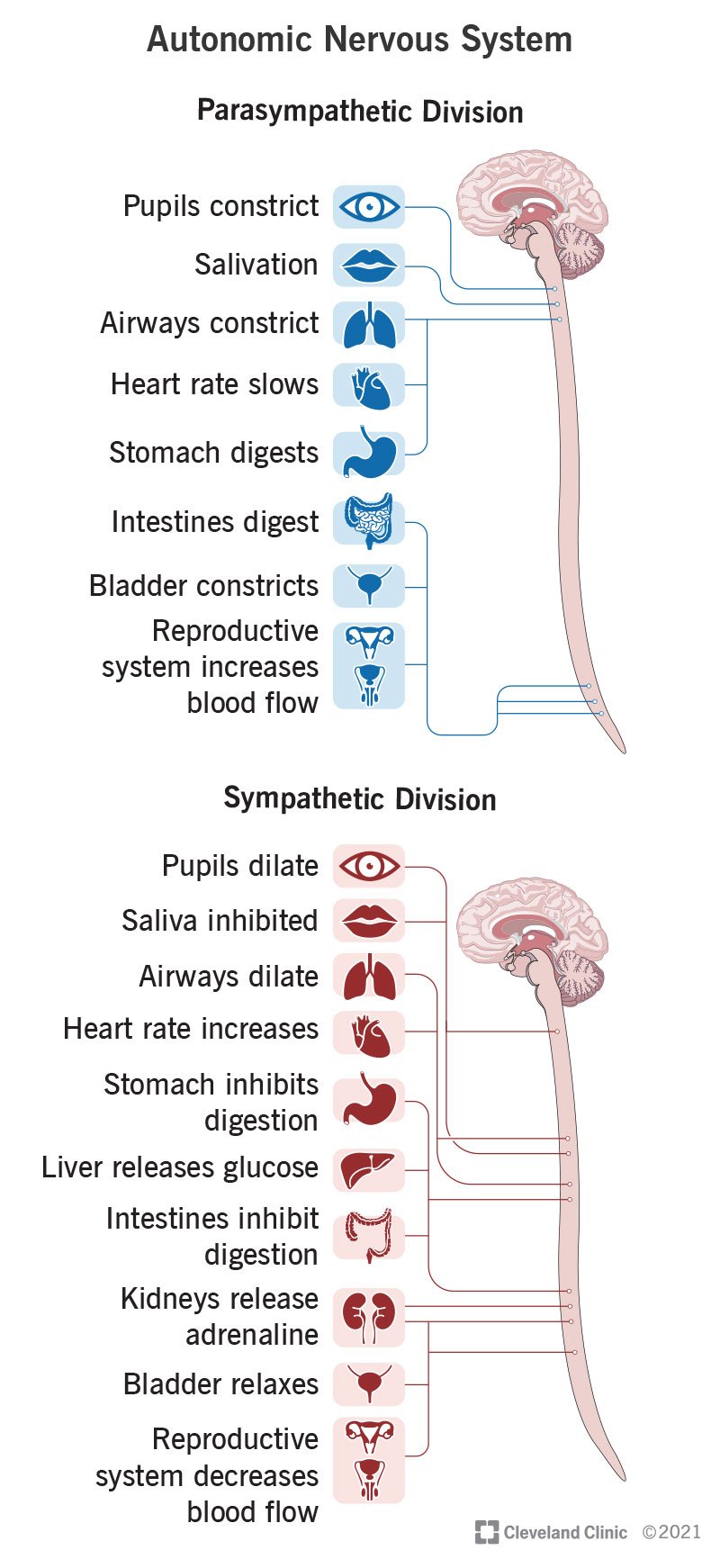
Autonomic Nervous System (Involuntary control):
Sympathetic nervous system:
Fight, flight and freeze
Parasympathetic nervous system:
Rest, digest, sex and read
12 Cranial nerves:
You do not need to memorise the full sequence in order, but you must understand the clinically relevant cranial nerves marked with a star below:
Somatic:
CN I – Olfactory (sensory)
*CN II – Optic (sensory)
*CN V – Trigeminal (facial sensation + chewing muscles)
*CN VII – Facial (facial expression muscles)
*CN VIII – Vestibulocochlear (hearing + balance)
*CN XI – Accessory (sternocleidomastoid + trapezius)
*CN XII – Hypoglossal (tongue movement)
Autonomic:
*CN III – Oculomotor (pupil constriction)
CN VII – Facial (salivary + lacrimal glands)
*CN IX – Glossopharyngeal (salivary gland)
*CN X – Vagus (major parasympathetic supply to heart, lungs, GI)
You must also be able to identify and explain which nerves are responsible for balance and taste.
Balance:
CN VIII – Vestibulocochlear
Taste:
CN VII – Facial
CN IX – Glossopharyngeal
CN X – Vagus
NB: Not all the cranial nerves are solely somatic or autonomic, most have dual somatic and autonomic functions.
2
PHYSIOLOGY
For physiology, you should be able to understand the underlying pathophysiology behind:
Consciousness and awareness:
Role of the cerebral cortex in cognition, awareness and higher function
Role of brainstem in maintaining alertness
Difference between focal neurological deficit and global impairment
Causes of unconsciousness – Remember the mnemonic FISH SHAPED:
F – Fainting (syncope):
Transient cerebral hypoperfusion
Vasovagal syncope
Simple syncope
Heart failure
I – Infections, for example:
Sepsis
Meningitis
Acute Disseminated Encephalomyelitis (ADEM)
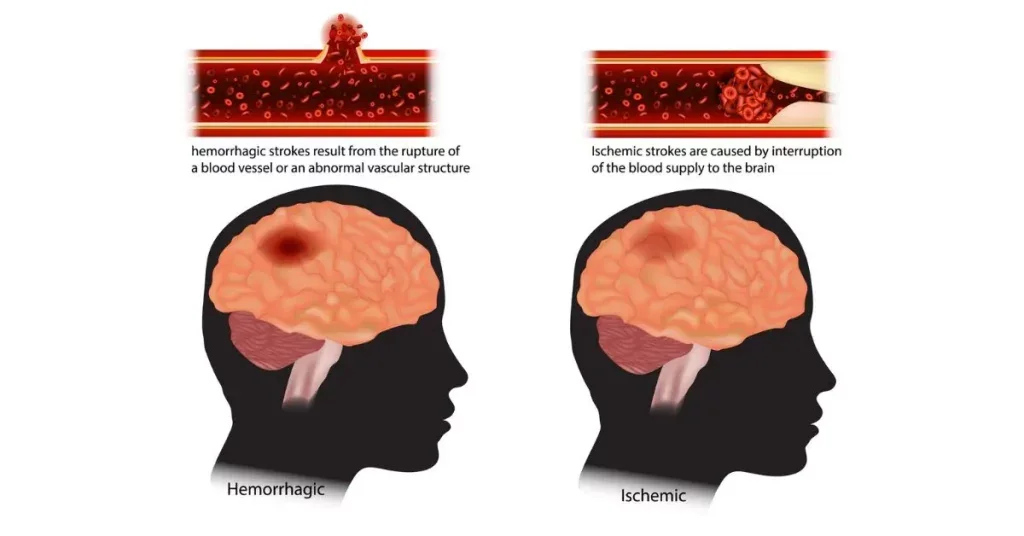
S – Stroke (Cerebrovascular Events - CVEs):
Ischaemic
Haemorrhagic
H – Head injury (Traumatic brain Injuries - TBIs)
Primary injury - Blunt force trauma, rapid deceleration etc
secondary injury - Hypoxia, hypotension, raised ICP etc
S – Shock
Reduced cerebral perfusion pressure
H – Hypoxia
Reduced oxygen delivery to brain tissue
A – Alcohol
CNS depression
P – Poisoning
Drugs, toxins, CO exposure etc
E – Epilepsy
Abnormal electrical cortical discharge broke into two categories:
Generalised seizures
Focal Seizures
D – Diabetes
Hypoglycaemia
Severe hyperglycaemia
You must understand the difference between:
Structural causes (bleed, tumour, stroke, trauma) and;
Metabolic/toxic causes (hypoxia, hypoglycaemia, drugs, sepsis)
Cerebral perfusion and oxygenation:
Cerebral perfusion pressure (conceptual understanding only)
Relationship between systemic blood pressure and brain oxygen delivery
Effect of hypotension on neuronal survival
Effect of hypoxia on neuronal survival
Loss of autoregulation in severe illness
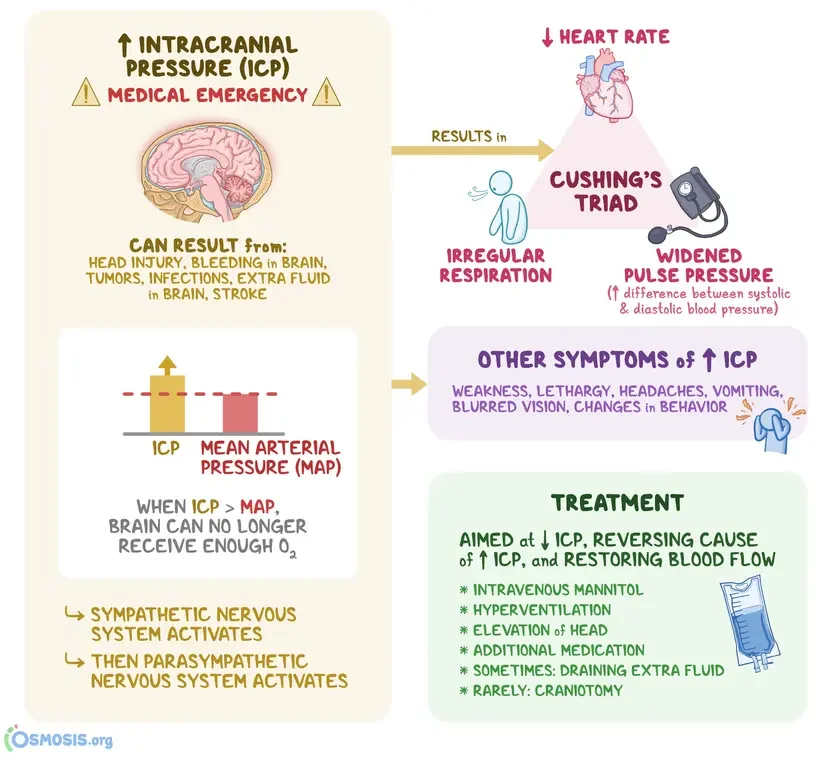
Intracranial pressure (ICP):
Monro-Kellie principle (fixed skull volume: brain tissue, blood, CSF)
Cushings response (Hypertension, Bradycardia, Bradypnoea)
Compensation vs decompensation
How bleeding, swelling or blocked CSF flow increases ICP
Consequences of raised ICP:
Headache
Vomiting
Reduced GCS
Unequal or non-reactive pupils
Abnormal posturing
Brainstem compression
Stroke pathophysiology:
Ischaemic stroke (thrombus vs embolus)
Haemorrhagic stroke
Transient ischaemic attack (TIA)
Penumbra concept (basic awareness only)
Large vessel occlusion (conceptual understanding)
Seizure physiology:
Abnormal electrical discharge in the cerebral cortex
Generalised vs focal onset
Post-ictal suppression
Risk of airway compromise
Spinal cord injury:
Disruption of ascending and descending pathways
Loss of sympathetic tone
Neurogenic shock
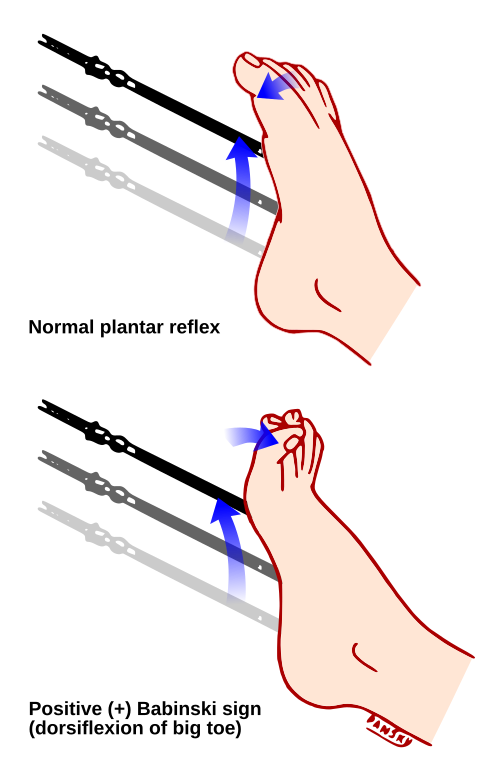
Babinski’s repsonse and priapism
Autonomic nervous system physiology:
Sympathetic activation
Parasympathetic dominance
Vagus nerve influence on heart rate
Autonomic instability in brainstem injury
Balance and coordination:
Role of cerebellum
Role of vestibular system (CN VIII)
Cerebellar stroke → ataxia, dysmetria, imbalance
Taste physiology:
Anterior 2/3 tongue – CN VII
Posterior 1/3 tongue – CN IX
Minor contribution – CN X
Infection of the nervous system:
Meningitis: meningeal inflammation → raised ICP → altered consciousness and possibly death
Encephalitis: inflammation of brain tissue → seizures → behavioural change → reduced GCS and possibly death
Acute disseminated encephalomyelitis: Immune-mediated demyelinating disorder, usually following viral infection → inflammatory response against CNS myelin → widespread demyelination → impaired nerve conduction → neurological deficit → altered consciousness.
You must understand the progression of:
Hypoxia or hypotension → reduced cerebral perfusion → confusion → reduced GCS → coma → cardiac arrest
Ischaemic stroke → vessel occlusion → ischaemia → infarction → cerebral oedema → raised ICP → deterioration
Intracranial bleed → expanding volume → increased ICP → brainstem compression → respiratory compromise → cardiac arrest
Meningitis → inflammation → raised ICP ± septic shock → multi-organ failure
Prolonged seizure → hypoxia → acidosis → exhaustion → post-ictal coma → airway compromise → possible death
For Level 5, you must be able to:
Recognise structural vs metabolic causes of unconsciousness
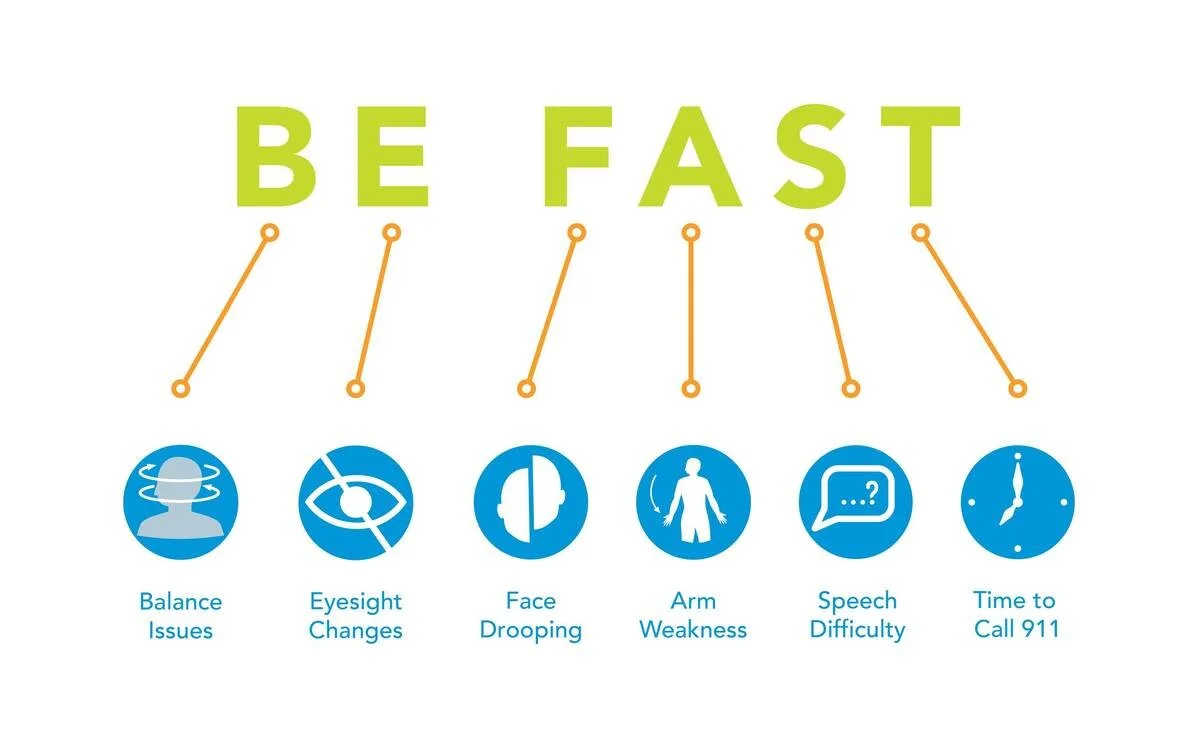
Identify time-critical stroke patterns using exams such as:
BEFAST Test
MEND Exam
HIT Exam
Understand why hypotension and hypoxia worsen brain injury
Protect the brain from secondary injury
Recognise early neurological deterioration before arrest occurs
Why do emt’s need to know this?
3
Altered level of consciousness is one of the most common and highest-risk presentations in prehospital care. Without understanding neurological physiology, assessment becomes guesswork.
GCS interpretation relies on knowing:
Which part of the brain controls eye opening
Which structures generate speech
Which pathways produce purposeful movement
Why a falling GCS indicates deterioration
Stroke assessment depends on understanding:
Why unilateral weakness occurs
Why facial droop happens
Why speech disturbance localises to specific hemispheres
Why posterior circulation strokes may present with imbalance rather than weakness
Why time equals brain
Recognising focal neurological deficit vs global impairment determines:
Stroke vs hypoglycaemia
Head injury vs intoxication
Sepsis vs intracranial bleed
Metabolic collapse vs structural brain injury
Unconsciousness assessment requires rapid application of FISH SHAPED to avoid missing reversible causes such as:
Hypoglycaemia
Hypoxia
Shock
Opioid toxicity
Cerebral perfusion knowledge explains:
Why hypotension worsens brain injury
Why hypoxia accelerates neuronal death
Why maintaining blood pressure and oxygenation prevents secondary brain injury
Understanding intracranial pressure allows you to recognise:
Cushing’s response
Unequal pupils
Abnormal posturing
Sudden deterioration after head injury
These directly influences urgency of transport and pre-alert decisions.
Head injury management depends on knowing:
Primary injury cannot be reversed
Secondary injury can be prevented
Airway, oxygenation and perfusion are neuroprotective
Seizure management requires understanding:
Why prolonged seizures cause hypoxia and acidosis
Why airway compromise is common
Why post-ictal states must not be mistaken for ongoing seizure
Spinal cord injury physiology explains:
Neurogenic shock (hypotension without blood loss)
Priapism as a sign of cord injury
Why immobilisation decisions matter
Autonomic understanding clarifies:
Bradycardia in raised ICP
Vagal influence on heart rate
Autonomic instability in brainstem injury
Balance and cerebellar function knowledge prevents:
Missing posterior stroke
Mislabelling neurological deficit as “vertigo” or anxiety
Infection-related neurology is time critical:
Meningitis and encephalitis can deteriorate rapidly
Sepsis can cause altered consciousness without focal deficit
Early recognition improves outcome
Differentiating between life-threatening and stable neurological presentations determines:
Treat and discharge
Treat and refer
Urgent ED conveyance
Blue light transport
Stroke centre pre-alert
Neurological deterioration can be subtle and rapid. EMTs must recognise:
Confusion before collapse
Behaviour change before reduced GCS
New imbalance before hemiparesis
Early stroke before complete deficit
Ultimately, neurological A&P allows you to answer three critical questions on scene:
Is the brain perfused?
Is the brain oxygenated?
Is this structural or metabolic?
If you can answer those confidently, you prevent secondary brain injury and improve survival and long-term neurological outcome.