

Chest Assessment in Pre-hospital Care: Medical and Trauma Approaches.
Figure 1: Chest auscaltation demonstration.
Chest assessment should always follow a structured clinical examination pathway in order to identify respiratory and thoracic conditions that may influence clinical decision making, including triage, treatment and transport. In pre-hospital emergency and urgent care practice, it helps clinicians recognise evolving chest conditions such as asthma, COPD, pneumonia, pulmonary oedema and pleural disease, while also identifying life-threatening traumatic chest injuries such as pneumothorax, haemothorax and diaphragmatic rupture. As with any focused examination, any deterioration should prompt an immediate return to the primary survey.
General principles before you start
Use a structured and repeatable sequence. Expose the chest adequately while maintaining dignity. Compare left with right and front with back wherever possible. Interpret all findings alongside the patient’s observations, mechanism of injury, history and overall presentation rather than relying on one isolated sign.
Chest assessment can be divided into two broad clinical contexts:
Medical chest assessment using IPPA (Inspect, Palpate, Percuss, Auscultate);
Trauma chest assessment using FLAPS TWELV (Feel, Look, Auscultate, Percuss, Search junctional areas, Tracheal deviation, Wounds, Surgical Emphysema, Laryngeal crepitus, Venous distension).
In either case, you are looking for two broad categories of clinical features:
Signs
Symptoms
Signs are the objective findings you observe, measure or elicit during assessment. In chest assessment, this includes respiratory rate, oxygen saturations, work of breathing, cyanosis, chest wall movement, percussion note and auscultatory findings.
Symptoms are the subjective features the patient reports experiencing. In chest assessment, this may include shortness of breath, chest tightness, pleuritic pain, cough, sputum production, wheeze, haemoptysis or orthopnoea.
Medical chest assessment
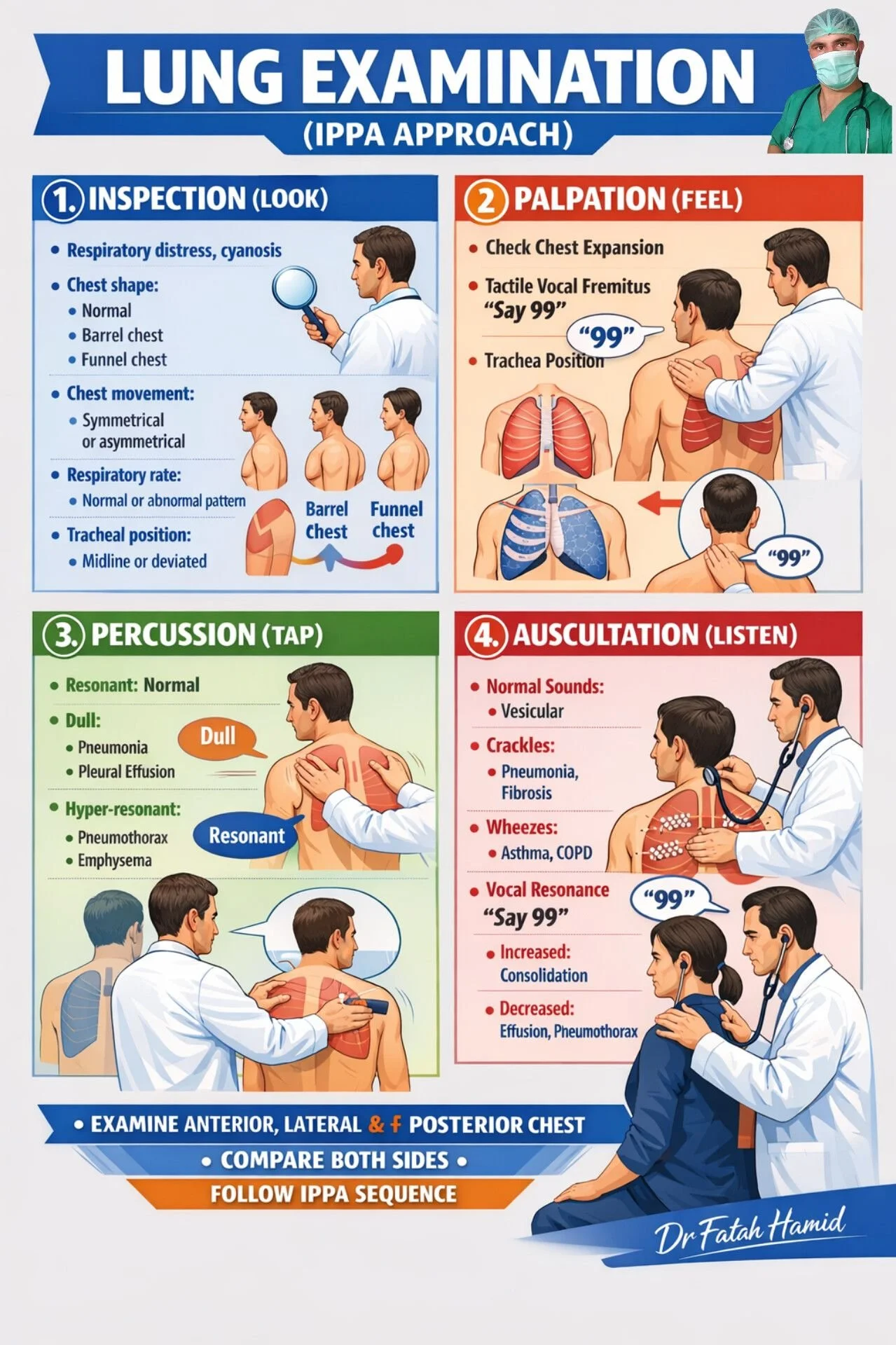
Figure 2: IPPA infographic.
Credit: Dr Fatah Hamid
Source: https://www.facebook.com/profile.php?id=100064390435547
Inspection
Inspection starts before you touch the patient. Introduce yourself by stating your name and clinical grade, but before approaching the patient, observe them closely to assess the Rate, Effort and Depth of their breathing, or RED if that helps you remember this part of the assessment. Observe whether the patient can speak in full sentences, whether they appear exhausted, whether they are tripodting, and whether they are using accessory muscles. Pursed-lip breathing, nasal flaring, intercostal recession and obvious distress are all important abnormal findings.
Next, approach the patient and record their physiological observations. Respiratory rate, oxygen saturations, heart rate, blood pressure, capillary refill time, temperature and level of consciousness all matter. You may also wish to measure blood glucose if the patient is diabetic, pregnant, has a reduced level of consciousness, or is displaying any neurological deficit.
In general, a full set of observations should be considered standard practice, particularly in the early years of clinical practice, until you are experienced enough to justify withholding specific measurements based on presentation. For example, a normally fit and well 18-year-old with an isolated sprained ankle may not require a blood glucose measurement. In many settings, a full set of observations may also include a 12-lead ECG where this is available, particularly in patients presenting with chest-related symptoms.
Once you have observed the patient from a distance and obtained a full set of observations, continue your inspection in a structured manner. At K2 International, we suggest the following sequence:
Start at the hands and assess for:
Clubbing of the nails. Digital clubbing is not a typical finding and should make you think more broadly about chronic suppurative or fibrotic lung disease, malignancy and, in some cases, COPD.
Asterixis, or a flapping tremor of the hands, should raise concern for severe hypercapnia or other metabolic disturbance.
Peripheral cyanosis may reflect hypoxaemia, poor perfusion, or both.
Tar staining, although not diagnostic, can support a smoking history and clinical context.
Move along the arm to the neck and assess for:
Jugular venous distension is worth identifying and documenting, as in the correct clinical context and with appropriate interpretation it may indicate raised central venous pressure, obstructive pathology or right-sided cardiac strain.
Cervical and supraclavicular lymphadenopathy or simply, raised lymph nodes around the neck, may suggest infection, inflammatory disease or malignancy and should not be missed in a proper chest assessment.
Then assess the face and mouth. Look for central cyanosis, poor dentition, oral candidiasis, mucosal lesions and obvious oral malignancy. In respiratory patients, this can help identify chronic disease burden, aspiration risk, inhaled steroid complications and alternative causes of symptoms.
Move down to the chest itself. Observe the breathing pattern using RED, then assess chest shape and symmetry for features such as:
Barrel chest,which may suggest hyperinflation and therefore an obstructive disease process such as COPD.
Pectus excavatum and pectus carinatum, which can alter normal thoracic mechanics and impair effective ventilation.
Kyphosis and scoliosis, which can also reduce effective ventilation by restricting thoracic expansion.
At the same time, note scars, deformity, asymmetrical movement and whether one side appears to lag behind the other.
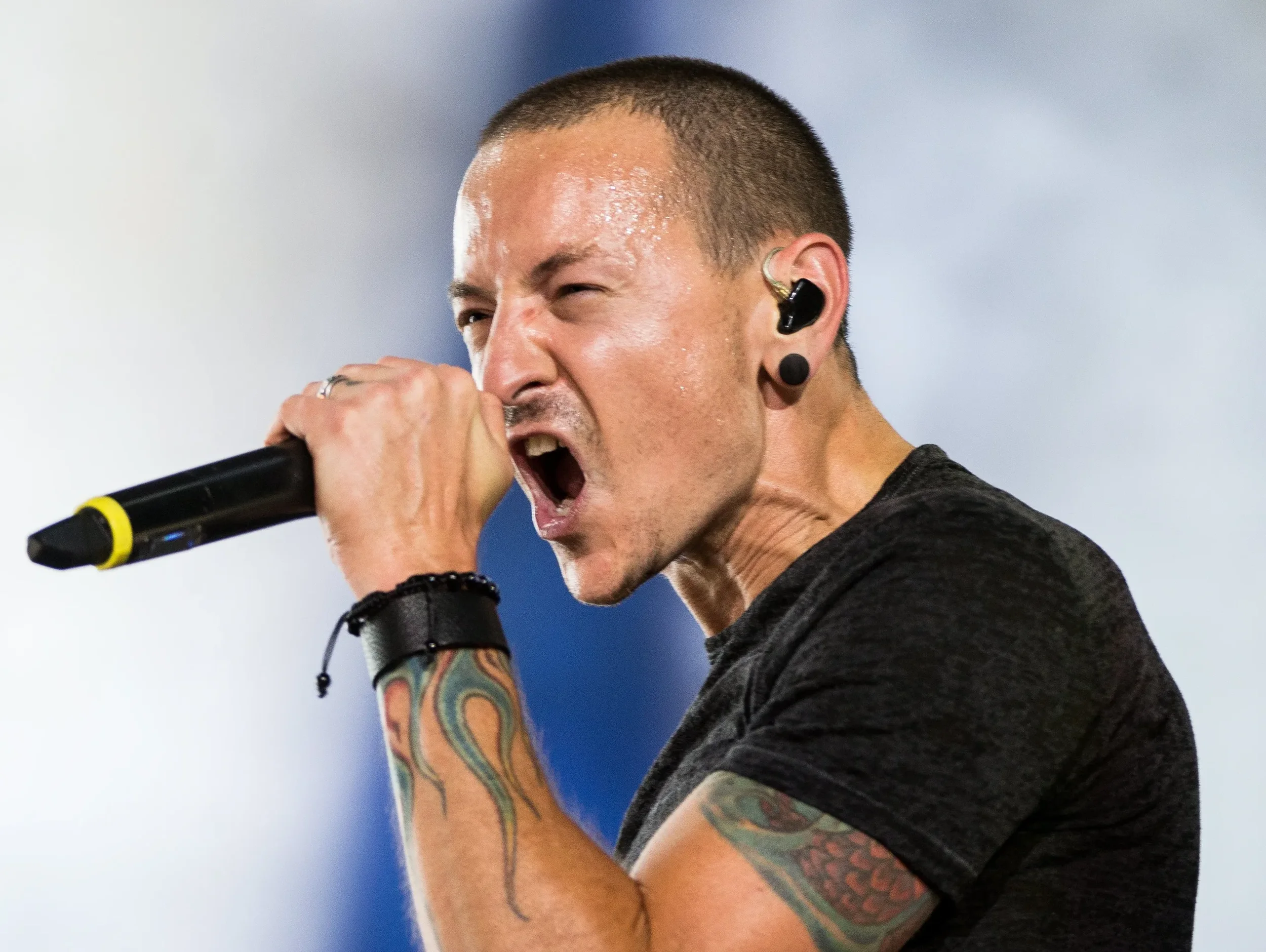
Figure 3: Chester Bennington displaying ‘Jugular Venous Distension’ as he is increasing his intrathoracic pressure when sustaining a note thus blocking the drainage of his jugular veins. An abnormal sign for a patient at rest, but completely normal for professions such as singers (when they’re signing that is).
Palpation
Palpation should assess for:
Tenderness.
Any pain on palpation may indicate previous trauma, occult fracture or costochondritis, which is inflammation of the costochondral cartilage.
Chest wall stability.
Assess for instability, deformity or crepitus, as these may indicate rib or sternal fracture. Reduced expansion on one side may point towards pneumothorax, pleural effusion, consolidation or pain-limited ventilation.
Equal bilateral rise and fall.
Assess whether the chest wall rises and falls equally on both sides during respiration.
Tactile fremitus.
This is the vibration felt through the chest wall when the patient speaks, often assessed by asking them to say “99” or “one, two, three”. It should normally feel symmetrical on both sides. Increased tactile fremitus suggests increased lung density, classically consolidation. Reduced tactile fremitus suggests a pleural process separating the lung from the chest wall, such as pleural effusion or pneumothorax.
At advanced level, this is also the point to consider whether tracheal position or apex beat assessment may be required, particularly if there is major unilateral pathology, marked asymmetry or concern for mediastinal shift. This is not always necessary in every patient, but it is often omitted when it may add significant clinical value.
Percussion
Percuss systematically and compare side to side, ideally in matched fields over the front and back. An eight-field approach front and back is sensible, provided it is performed consistently and you compare like with like.
Normal lung is resonant. This is a skill that improves with experience, so it is important to practise percussion on as many appropriate patients as possible in order to develop an ear for what normal resonance sounds like.
Hyper-resonance raises suspicion of pneumothorax or hyperinflation. In simple terms, it sounds louder and more hollow than normal, suggesting an abnormally increased volume of air beneath the area being percussed.
Hypo-resonance or dullness suggests denser underlying tissue or fluid, such as:
Consolidation. This occurs when the lung tissue becomes filled with fluid, pus or other material, producing a dull percussion note. Consolidation also tends to increase tactile fremitus because sound is transmitted more effectively through denser lung tissue. Clinically, this may indicate pathology such as pneumonia and, in some cases, malignancy. The wider history and examination findings should guide your index of suspicion. For example, a short history of productive cough and fever may point towards pneumonia, whereas progressive shortness of breath, weight loss and a more prolonged history may raise concern for malignancy.
Haemothorax. Blood within the pleural space produces a dull percussion note and typically reduces tactile fremitus, as the fluid separates the lung from the chest wall.
Pleural effusion. A collection of fluid within the pleural space between the visceral pleura and parietal pleura also produces a dull percussion note and usually reduces tactile fremitus for the same reason.
These findings should always be interpreted alongside the rest of the assessment, particularly chest expansion, tactile fremitus and auscultation, to help determine whether the pathology is within the lung tissue itself, such as consolidation, or within the pleural space, such as haemothorax or pleural effusion. Auscultation helps build the picture, but pleural effusion is confirmed with imaging rather than examination alone.
Auscultation
Auscultate the same fields you percussed, again comparing side to side and like with like. Listen not just for the presence of sound, but for symmetry, intensity and the phase of breathing in which the abnormality occurs. Reduced or absent breath sounds may reflect poor effort, severe airflow limitation, pleural effusion, pneumothorax, obesity or hyperinflation. Below are some common sounds that pre-hospital clinicians must be able to identify and interpret:
Wheeze. Wheeze is a high-pitched sound caused by narrowed airways and is commonly associated with asthma, COPD, airway obstruction or mucus plugging. To interpret this finding further, you must decide whether the wheeze is predominantly expiratory, inspiratory, or present in both phases of respiration.
Expiratory wheeze. Expiratory wheeze is the most common type of wheeze detected by ambulance staff. This is usually indicative of obstructive pathophysiology such as bronchospasm, which is common in asthma, COPD and some lower respiratory tract infections. It occurs because air is moving through narrowed lower airways, producing a higher-pitched musical sound.
Inspiratory wheeze. Inspiratory wheeze should prompt careful consideration of upper airway involvement. In many cases, a high-pitched inspiratory sound is more accurately described as stridor, which may indicate upper airway narrowing caused by foreign body obstruction, swelling or a mass. This is clinically important, as upper airway pathology carries different risks and management priorities to lower airway disease.
Inspiratory AND expiratory wheeze sometimes described as biphasic wheeze, may occur when there is more severe or fixed central airway narrowing. This can be caused by significant airway swelling, a foreign body or a mass affecting the trachea or main bronchi. In some patients with worsening asthma or COPD, wheeze may also become more widespread as airflow limitation becomes more severe.
Fine crackles are usually associated with alveolar or interstitial pathology such as pulmonary oedema and pulmonary fibrosis. They are typically heard on inspiration and are thought to reflect the sudden opening of small airways and alveoli, often in the presence of fluid or interstitial change.
Coarse crackles. Coarse crackles suggest secretions within the larger airways and are more in keeping with bronchiectasis, pneumonia, pulmonary oedema or heavy mucus burden. They are lower in pitch than fine crackles and may change after coughing.
A pleural rub, although less common, suggests inflamed pleural surfaces rubbing together and should be actively considered in pleuritic presentations. This can sound like creaking leather and is often associated with pain on inspiration.
Do not forget vocal resonance. Bronchophony, egophony and whispered pectoriloquy all reflect increased sound transmission through denser lung tissue or fluids. In practical terms, they support a diagnosis of consolidation, although egophony may also be heard at the upper border of a pleural effusion. These findings should always be interpreted alongside the patient’s history, physiological observations and overall clinical picture.
Bronchophony is an increase in the clarity and loudness of the patient’s spoken voice when listening with a stethoscope over the chest. Ask the patient to say “ninety-nine” or “one, two, three”. Normally, the words sound muffled, but over an area of lung consolidation they become clearer and louder. This is most commonly associated with pneumonia.
Egophony is an abnormal change in voice sound heard during auscultation. Ask the patient to say “ee”. If it sounds more like “ay”, this is a positive finding. It happens when sound is altered as it passes through abnormal lung tissue and is classically associated with consolidation, and can also be heard just above a pleural effusion.
Whispered pectoriloquy is present when whispered words are heard clearly through the stethoscope. Ask the patient to whisper “one, two, three” or “ninety-nine”. Normally, a whisper is faint and indistinct, but over consolidated lung it becomes unusually clear. Like bronchophony, it suggests increased sound transmission through dense lung tissue, such as pneumonia.
What pre-hospital clinicians often miss during an IPPA assessment
A good chest assessment is not just deciding whether the chest sounds clear or noisy. Clinicians often miss the hands, the neck, the lymph nodes, chest shape, the expiratory phase, vocal resonance and the clinical importance of gaining and interpreting a full patient history. Those additional findings are often what turn a generic respiratory examination into a genuinely specialist assessment.. A few common examples of patterns are listed below:
-
Inspection: A 38-year-old female has presented to you while you are working in an OOH GP service with a 1 week history of feeling generally unwell, aching joints, productive cough and intermittent fever and a NEWS2 score of 3 due to mild tachycardia and pyrexia. This is her first ever attendance to a primary care service and she is normally very fit and well.
Palpation: Increased tactile fremitus noted over left lower lobe only. No other abnormalities detected.
Percussion: Dullness to percussion or hypo-resonance noted over the left lower lobe only. All other fields were resonant.
Auscultation: Crackles heard over the left lower lobe with increased vocal resonance, including positive bronchophony and whispered pectoriloquy. Breath sounds are reduced over the affected area.
-
Impression: Lower respiratory tract infection, most likely pneumonia.
-
Inspection: In this instance, we have a relatively young woman with no known past medical history and a short history of symptoms which are more suggestive of an acute infection than a chronic disease process. Her productive cough, intermittent fever, systemic symptoms and mildly raised NEWS2 score all support this. While more serious pathology can never be completely excluded on first presentation, the history makes an infective process a reasonable working diagnosis. Clinical history is often the most important contributor to diagnosis, but it must always be interpreted alongside examination findings and, where required, further investigation.
Palpation: In this instance, increased tactile fremitus has been identified over the affected area. This suggests increased transmission of vibration through denser underlying lung tissue. In the context of this patient’s history, this supports consolidation rather than a pleural process such as pleural effusion or pneumothorax, both of which would be expected to reduce tactile fremitus.
Percussion: In this instance, dullness to percussion is present over the left lower lobe. This suggests that the normal air-filled lung beneath the percussion point has been replaced or obscured by denser material. In the context of this history and the palpation findings, this is again supportive of consolidation, most likely caused by infection.
Auscultation: In this instance, positive bronchophony and whispered pectoriloquy indicate increased transmission of sound through denser lung tissue, which is a classic feature of consolidation. The crackles over the affected area further support alveolar or airway involvement in an infective process. Reduced breath sounds may also occur over the affected region depending on the extent and nature of the underlying pathology. Taken together with the percussion and palpation findings, the auscultation findings strongly support left lower lobe consolidation.
Conclusion: In a patient with a short history of productive cough, intermittent fever and systemic upset, alongside physiological evidence of infection and examination findings consistent with focal consolidation, it is reasonable to conclude that this patient has a lower respiratory tract infection, most likely pneumonia. Pneumonia is more likely than acute bronchitis in this case because there is evidence of focal consolidation, which would not be expected in uncomplicated bronchitis.
-
Inspection: A 68-year-old male has contacted his GP surgery with shortness of breath that has been worsening over several years and the receptionist has referred him to 999. He appears cachectic and reports losing several stone over the past 6 months. You note digital clubbing and an enlarged left supraclavicular lymph node. He also reports a diagnosis of gastric cancer 3 years ago. His observations reveal a NEWS2 score of 0 at rest.
Palpation: Increased tactile fremitus noted over the left lower lobe only. No other abnormalities detected.
Percussion: Dullness to percussion noted over the left lower lobe only. All other fields appear resonant.
Auscultation: Breath sounds are reduced over the left lower lobe with increased vocal resonance, including positive bronchophony and whispered pectoriloquy. All other fields have normal vesicular breath sounds.
-
Here, we have two patients with remarkably similar IPPA findings. Crucially, the deciding factor is their history. Remember, a patient’s history often forms the largest part of the diagnostic picture.
In both examples, the patients demonstrate examination findings consistent with focal consolidation in the left lower lobe.
However, patient 1 has a short history, physiological features suggestive of infection, and examination findings consistent with consolidation. In this context, it is reasonable to suspect a lower respiratory tract infection, most likely pneumonia, and manage accordingly.
Patient 2, however, has no physiological signs of acute infection and has a concerning history, including chronic progressive symptoms, cachexia, weight loss, clubbing and supraclavicular lymphadenopathy. In this context, the same focal examination findings should raise suspicion of an underlying malignancy rather than simple infection. This patient therefore requires urgent further investigation via the appropriate suspected cancer pathway, rather than empirical treatment alone.
Another way to support clinical decision making may be point-of-care blood testing, if available. In patient 1, a point-of-care CRP may help guide antibiotic prescribing if it is unclear whether antibiotics are needed for a lower respiratory tract infection, but it should not be used in isolation to diagnose pneumonia. In patient 2, blood tests may contribute to the wider clinical picture, but they do not rule malignancy in or out. In practice, the history, examination findings and urgent imaging or referral pathway are more important than ESR when malignancy is suspected.
-
Inspection: This patient has several red flag features for malignancy. He has a history of gastric cancer, significant unexplained weight loss, digital clubbing and an enlarged left supraclavicular lymph node. An enlarged left supraclavicular node, often referred to as a Virchow node, is classically associated with metastatic malignancy, particularly from abdominal malignancy such as gastric cancer. Taken together, these findings should significantly raise suspicion of an underlying malignant process rather than simple infection.
Palpation: This patient has increased tactile fremitus over the left lower lobe, which suggests increased transmission of vibration through denser underlying lung tissue. This is more in keeping with pulmonary consolidation than with pleural effusion or pneumothorax, both of which would be expected to reduce tactile fremitus.
Percussion: Dullness to percussion over the same area supports the presence of denser underlying tissue replacing normal air-filled lung. In the context of the palpation findings, this again supports focal consolidation. On its own, however, percussion cannot distinguish whether that consolidation is caused by infection, malignancy or another pathology.
Auscultation: Reduced breath sounds with positive bronchophony and whispered pectoriloquy suggest increased sound transmission through abnormal dense lung tissue, again supporting focal consolidation. When these findings are combined with the patient’s concerning history and inspection findings, the overall picture is suspicious for an underlying malignant process affecting the left lower lobe, either as a primary lung malignancy or metastatic disease. This patient therefore requires urgent further investigation via the appropriate suspected cancer pathway rather than empirical treatment alone.
Figure 4: Geeky Medics instructional video on how to percuss, palpate and auscultate the chest.
tRAUMA CHEST ASSESSMENT
In trauma, chest assessment must remain fast, deliberate and integrated with the primary and secondary survey. It should identify immediately life-threatening thoracic injury without becoming a slow, overly academic exercise. The FLAPS TWELV approach works well because it is practical, easy to teach and easy to remember even in an emergency situation.
FEEL
Using both hands, assess the sternum, anterior chest, lateral chest, axillae and as much of the posterior thorax as the situation safely allows without rolling the patient if you suspect spinal involvement (Don’t forget projectiles that have cross the patient’s mid-line should be considered a spinal injury even if there are no obvious neurological deficits evident).
Feel for tenderness, instability, crepitus, paradoxical movement and asymmetrical chest rise.

Figure 5: Dr Scott McKee - MIRA graduate and K2 instructor performing the “the FEEL & LOOK” part of FLAPS TWELV in a trauma scenario.
LOOK
Expose the patients chest by cutting off any clothes, armour or protective clothing they may be wearing. If done correctly, the patient’s clothes should essentially be “butterfly’d” around them. For example, for a t-shirt you could use your trauma sheers to cut a ‘Y’ shape which will allow you to expose the patient’s chest fully without rolling them.
Once the patient is exposed, look for the following:
Tracheal deviation: A very late sign of tension pneumothorax. If the patient’s trachea has visible deviation, they are experiencing mediastinal shift meaning chest decompression via needle thoracocentesis or surgical thoracotomy is required immediately.
Wounds: Assess the chest, neck, and junctional areas such as around the neck/collar area and both axillae for wounds, especially penetrating wounds. For junctional areas where you are unsure there is chest injury involvement: if it’s bleeding - pack it, if its not - seal it. Bleeding likely indicates a neck or limb injury rather than a chest injury, but there may be overlap. The key takeaway is that you must not pack the chest cavity.
Surgical emphysema: Indication of air trapped in the soft tissues surrounding the neck and chest. If paired with recent trauma, indicates major trauma of the chest and should increase index of suspicion for further, multi-system trauma.
Laryngeal crepitus: Crepitus or feeling of hard tissues rubbing together when the larynx (voice box or ‘Adams Apple’) indicating significant trauma to the throat and that advanced airway intervention such as intubation (likely via RSI) or surgical airway is required.
Venous distension: Distension of the jugular veins (where they are obviously visible like when a professional singer sustains a note like in figure 3) either side of the neck.
Evaluate: all your signs and symptoms you have found so far and decide if needle thoracocentesis is required (reduced GCS paired with any of the above in major trauma).
Auscultate
If the environment allows it, assess for equal bilateral air entry and exit. Reduced or absent air entry on one side in trauma should be taken seriously. In the right context it supports pneumothorax, haemothorax or major parenchymal injury. If bowel sounds are heard in the chest, diaphragmatic rupture with herniation of abdominal contents must be considered.
Percuss
This step often isn’t possible due to ambient noise, but if possible assess for the following:
Hypo-resonance: If combined with reduced air entry over the same area, suspect haemothorax and prepare for finger or tube thoracostomy if trained and authorised to do so or to assist a senior clinician.
Hyper-resonance: if combined with reduced air entry over the same area, suspect pneumothorax or tension pneumothorax if paired with any other symptoms from the TWELV mnemonic and prepare for needle thoracocentesis immediately.
As with medical examination, percussion is strongest when combined with the results of a robust auscultation.
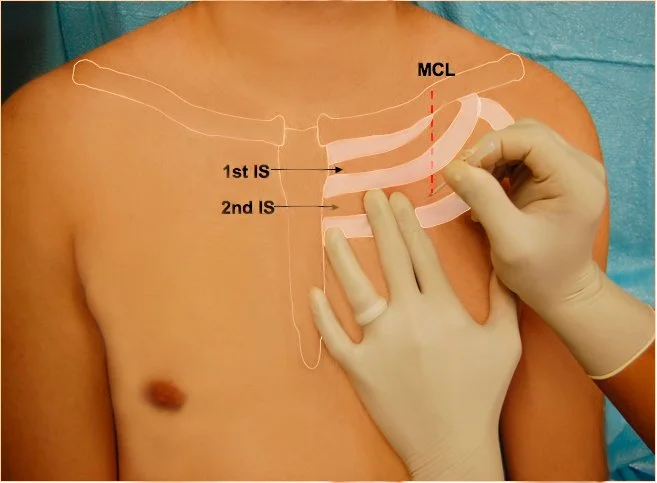
Figure 6: Needle thoracocentesis placement diagram.
Source: https://e-gcrme.com/gcrme/pedi_trauma/management/Needle_Thoracostomy.php
Search
Search the collar line, axillae, upper back and neck carefully. These are easy places to miss penetrating wounds. Junctional wounds can sit close enough to the thorax to create diagnostic uncertainty, so this stage matters. Your existing wording is good here: if it is bleeding, pack it; if it is not, and it is clearly thoracic, seal it. The key point is that you do not pack the chest cavity.
TWELV findings explained
Tracheal deviation is a classic but late sign of tension pneumothorax and should never be waited for before acting.
Wounds may indicate open pneumothorax or deeper thoracic penetration.
Surgical emphysema suggests air has escaped into the soft tissues and should raise concern for major chest or airway injury.
Laryngeal crepitus suggests significant laryngeal or upper tracheal trauma.
Venous distension may support obstructive physiology such as tension pneumothorax, but it can be absent, particularly in hypovolaemic trauma patients.
One important caveat is that the classic signs of tension pneumothorax are not especially sensitive. Their absence does not exclude tension physiology. In practice, mechanism, respiratory distress, unilateral findings, falling saturations, worsening haemodynamics and overall patient appearance matter more than waiting for a perfect textbook picture.
CONCLUSION
A proper chest assessment is one of the highest-yield focused examinations in pre-hospital care. In medical presentations, IPPA gives you a structured way to link symptoms, observations and examination findings to likely respiratory pathology. In trauma, FLAPS TWELV provides a rapid method of identifying immediately dangerous chest injury.
In both contexts, the aim is the same: recognise the sick patient early, identify the likely pathology, and make better treatment and transport decisions.
further reading
FirstAidForFree.com (no date) First aid mnemonics: handy reminders. Available at: https://www.firstaidforfree.com/first-aid-training-resources/first-aid-mnemonics/
Ferguson, CM (1990) Inspection, auscultation, palpation, and percussion of the abdomen. In: Walker, HK, Hall, WD, and Hurst, JW (eds) Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd edn. Boston: Butterworths. Available at: https://www.ncbi.nlm.nih.gov/books/NBK420/
Rescue Academy EMS (2022) Needle decompression tension pneumothorax [YouTube short]. Available at: https://www.youtube.com/shorts/FQC4qaQkB1E
Disclaimer: This guide is provided for educational purposes only. It is not a substitute for certified first aid training. Although we base our information on current UK-approved guidelines (Resuscitation Council UK, St John Ambulance, etc.), performing first aid requires practice, training and judgement. If in doubt, always call emergency services (999 in the UK) and wait for professional responders. K2 International does not accept liability for actions taken by users based on this guide.